My Cancer on MyChart
By Eric Perakslis, PhD
Providing patients with immediate access to their health data as it becomes available is a big step forward for transparency and patient empowerment, but the potential for unleashing a flood of information without sufficient context and support also carries risks.
My cancer is back, but no complaints—I’ve been managing renal cancer intermittently since 2006. I’m lucky in that my life remains normal and rich. This time is different, however, as I suffered serious side effects during treatment and a second, different primary cancer that will need investigation, staging, and (maybe) treatment was also found.
Looking back, the most significant technological change between my prior experience and my current one has been the evolution of MyChart, the patient portal offered by healthcare systems using the EPIC electronic health record (EHR). This time around, MyChart provided an almost real-time view of my cancer journey. But as recently detailed by the New York Times, the pros and cons of providing patients with immediate access to the results of medical test results are complex and controversial. As someone who studies the benefits and risks of health technologies, I’d like to offer my own story and take on the issues.
Transparency and its Tribulations
Recently enacted federal regulations have mandated that patients be given full access to their medical records. This is a significant step forward in healthcare transparency and patient empowerment. However, as with many new technologies, the benefits seem clear while the downsides are less obvious. Some examples of the latter were clearly articulated in a recent academic debate when Aaron Shapiro, who at the time was completing an internal medicine residency, described how his mother learned she had cancer through an automatically released pathology report. Dr. Shapiro rightly noted the lack of preparation of all parties involved. There was no training for clinicians, no notice or instructions to patients— just data pushed automatically to a patient who had no warning or idea what to do when she received an email telling her she had cancer. The resulting counterpoint is exactly what I would expect of technocentric health regulators: “educational…webinars were held”… “patients have the option not to log in and read”…
In other words: we did our job; it’s now up to you doctors and patients to figure it out. Even though public input included requests for these kinds of transparent capabilities, this answer strikes me as just another example of unhelpful and potentially dangerous public health messaging. We can do better.
My personal MyChart story began with my annual MRI scan on July 14 of this year. My appointment time was 10 AM; the results arrived less than 4 hours later. The report informed me that my cancer was back. It would be another week before I heard from my oncologist (not her fault). This same dynamic played out repeatedly as my MRI led to treatment, the treatment led to side effects, and the side effects led to an extended emergency room stay. Each step of the way, my phone would buzz with the latest test result…and I had to look. Lying on a bed in the hallway of an overburdened emergency room along with dozens of other patients, I had my data well before the busy medical staff did.
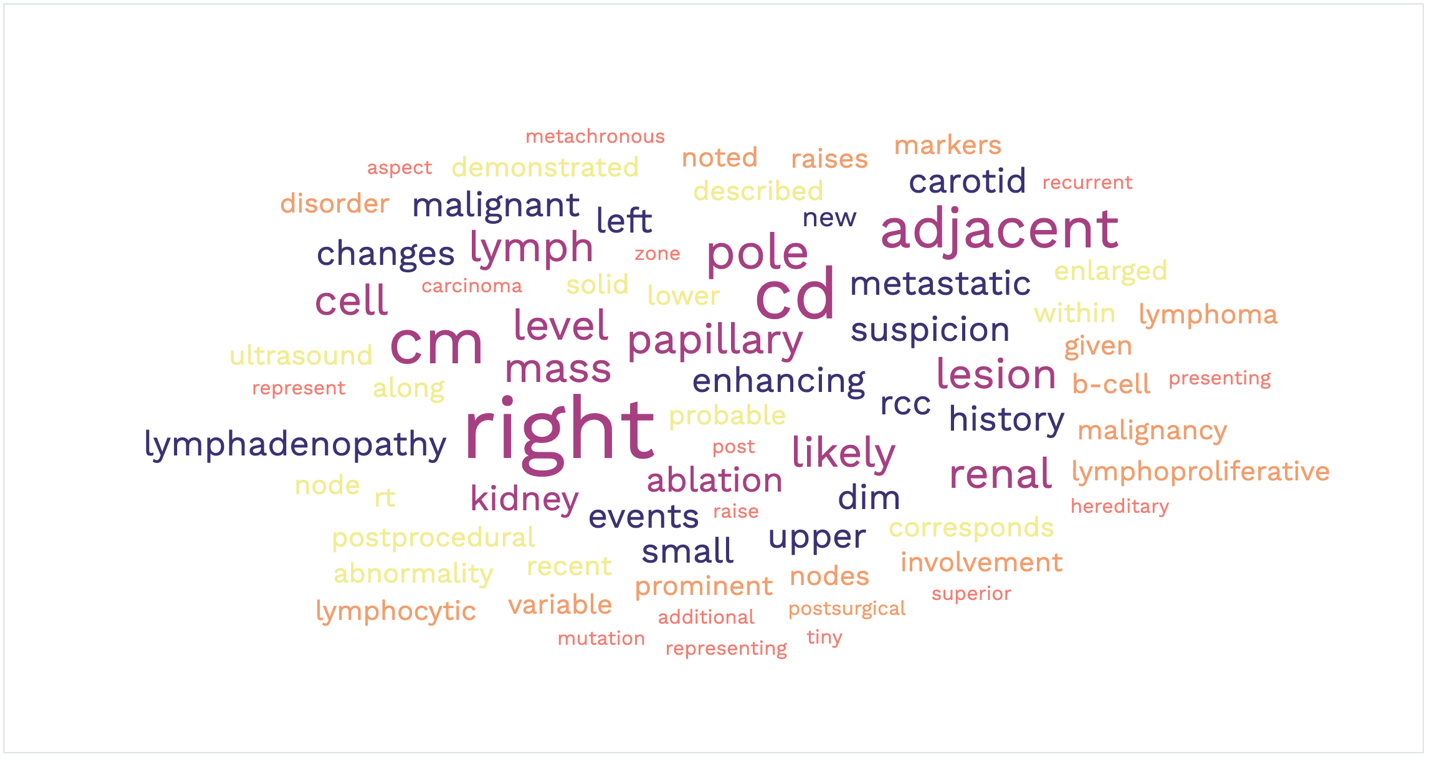
From July through early November, my MyChart posted the results of 21 different medical tests, almost all of which were delivered within hours. The word cloud above is the result of me aggregating the technical terms within these reports. I can’t help imagining the average person, without any scientific background or training, scouring the internet trying to answer their own questions as they wait days and weeks before seeing their healthcare provider.
Of course, MyChart offers multiple other benefits for patients. Tracking appointments is fantastic, and advance check-in and the ability to pay co-pays in advance is also helpful. Appointment reminders are more hit-or-miss, as the MyChart, phone calls, and SMS reminders often carry contradictory messages and instructions, but they will figure that out someday. I appreciate the transparency this information provides. Still, as someone who studies the benefits and harms of medical technologies, I believe the potential downsides are also clear.
First, there are misinterpretations and misunderstandings that can lead to unnecessary tests, exposure to unreliable sources, and potentially dangerous treatments. Second are misinformation and disinformation exposures, recently described as a leading cause of death by FDA Commissioner Robert Califf. The same online adversaries who oppose vaccination and mask wearing are happy to sow distrust in science and medicine on other medical fronts, and we know these campaigns are highly effective and resilient to countermeasures. Third, extensive online searching of medical terms leads to a greatly enhanced personal cyber attack surface (this in short is all of the points through which an online attacker can enter your digital life), which equates to increased cybersecurity vulnerability. Other convenience elements of MyChart, such as email, text, and phone reminders and notifications, also greatly increase patient cyber vulnerability. Fourth and finally are the inevitable negative psychological effects of receiving frightening information out of context without the necessary expertise for proper interpretation.
Doing Better as We Move Forward
We can do better. We must do better. We need to absorb lessons from biomedical research, where the best ways to return research results to participants have been studied thoroughly. According to a study from the National Academies of Science, Engineering and Medicine (NASEM), the benefits of research participation and transparency must be balanced through proper preparation, policy development, and adequate resourcing. A second NASEM report sponsored by multiple agencies within the Department of Health and Human Services (HHS) agencies also addressed the potential for poor decision-making by patients and adverse psychological effects. Interestingly, both reports recommend careful communication and education of clinicians and research participants on the benefits and risks of receiving study results.
Unfortunately, none of this has happened in healthcare before, during, or after the changes in MyChart. Instead, patients receive texts and emails informing them that their test results are ready, and are led to a list of test results with only a sidebar warning, such as the one shown here.
This is not nearly good enough. The American Medical Association (AMA) has decried the harms associated with such an approach and claimed that 65% of patients would prefer to speak to their medical professional before receiving results. In their view, the best solution is to modify regulations to allow the withholding of certain information until the clinician can communicate with the patient. My concern with this solution is that the resulting reduction in transparency will likely be permanent—but such an outcome is unnecessary when there are other fixes.
First, the process of providing test results to patients should be explained at the time those tests are prescribed. Clinicians already take the time to explain procedures to patients—a few more minutes discussing the return of results would save downstream time lost to frantic phone calls, expedited appointment requests, and MyChart message overload. If the clinician senses disproportionate stress (such as suicidality), they can take steps to ensure that support is available to the patient.
Second, similar information could be provided as part of the consenting and registration process when performing diagnostic procedures that include the risk of communicating troubling information. Third, each report should include some form of expert explainer that reminds the patient that the information contained in the report, if taken out of context of the rest of their medical history, could lead to misconceptions and misunderstandings. Lastly, reports could include links to appropriate patient navigation resources that could offer training in managing these conversations. All of these communications should also include a brief overview advisory on the potential dangers of internet research.
To be clear, I am absolutely not implying that all these communications should result in additional burdens for clinicians. Instead, I’d strongly suggest that healthcare institutions build time for these important conversations into the framework of the “standard” patient visit. The statistics on clinician burnout are mostly going unheeded by health systems, some of which are struggling financially while others are posting profits in the billions of dollars. The figure at right is taken from the Agency for Healthcare Research and Quality (AHRQ). While oversimplified, it shows how the instant return of results to patients likely exacerbates time pressure, inflates the amount of clinician time taken by EHR/MyChart, and contributes to a chaotic clinical environment.
Relieving these pressures on patients and clinicians may sound expensive, but not doing so will be far more costly. Given that healthcare is the leading cause of bankruptcies in the United States, the fact that public trust in healthcare is declining, and the news is replete with a steady stream of high-profile stories describing controversial uses of patient data, investments in better patient communication and engagement are both essential and overdue.

Having completed treatment for my recurrent renal cancer, I’m now in the early phases of having my newly diagnosed chronic lymphocytic leukemia (CLL) subtyped so we can plan treatment. My amazing medical oncologist has been juggling my referral to a CLL expert via text and MyChart messages while she is away on holiday. My new CLL specialist has sent me his email so I don’t get lost in the chaos of the health system. I could not be more thankful to them or the precious few support staff that try to keep their lives sane while ensuring patients are getting necessary care. They are my and my family’s heroes.
Googling the terms in my personal cancer word cloud quickly reveals the best and the worst medical information the internet can offer. The only constant is that all of it is out of context with my individual situation. I don’t agree that the regulations should be rolled back or modified to decrease data transparency. This is progress—lumpy, bumpy, imperfect progress. If we do roll back these regulations, we will never get this level of transparency again. Instead, we need to move forward. Enormous amounts of data is being pushed out to patients as I write this. Let’s take the necessary steps to enhance the benefits and mitigate the risks.

Eric Perakslis, PhD, is Science & Digital Officer for Duke Clinical Research Institute, Chief Research Technology Strategist for the Duke University School of Medicine, and a professor in the Department of Population Health Sciences, Duke University School of Medicine.